Knee Osteoarthritis
A summary of knee osteoarthritis and what can be done to help it, including the role of steroid injections.
Dr Peter Weil (GP), Claire Weil (RN)
1/2/20264 min read
Knee pain from osteoarthritis is one of the most common reasons people seek medical care. Osteoarthritis occurs when the cartilage in the knee joint gradually wears down, leading to pain, stiffness, and reduced mobility.
This condition affects millions of people and can significantly impact daily activities, from walking and climbing stairs to enjoying exercise and hobbies.
This brief guide explains:
What causes knee osteoarthritis
The options to treat it
How steroid injections can help — including how often they work and when they don't.
What Is Knee Osteoarthritis?
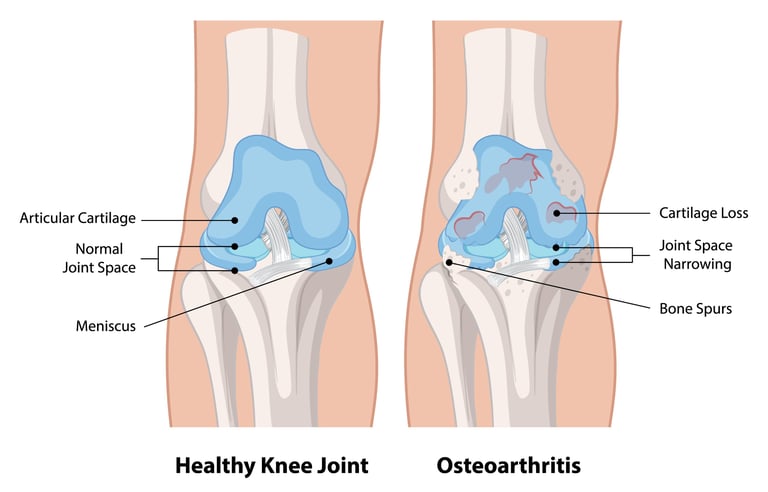
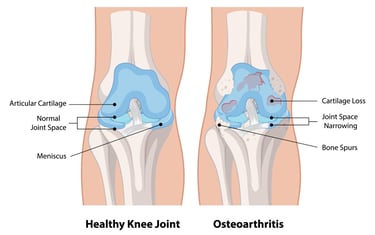
Osteoarthritis is a condition where the protective cartilage that cushions the ends of bones gradually wears away. In the knee, this breakdown leads to bone rubbing on bone, inflammation, and pain. The body often responds by developing bone spurs (osteophytes) and the joint can become swollen and stiff.
Common symptoms are:
Pain with activity, especially walking, standing, or climbing stairs
Stiffness, particularly after rest or first thing in the morning (usually less than 1 hour)
Swelling around the knee joint
Reduced range of movement
A grinding or clicking sensation (crepitus)
Difficulty bearing weight on the affected knee
The main risk factors include age, previous knee injuries, being overweight, genetics, and repetitive stress on the joint. Women are more commonly affected than men, especially after menopause.
How Is It Diagnosed?
Diagnosis typically involves discussing your symptoms and medical history, followed by a physical examination. Your clinician will assess pain, swelling, range of motion, and joint stability. X-rays are often used to confirm the diagnosis and assess the severity of joint damage, showing joint space narrowing, bone spurs, and other changes. In some cases, MRI scans may be used to evaluate soft tissue damage, as X-rays do not show this well.
What Are the Main Treatments?
Exercise and Physiotherapy - Strengthening the muscles around the knee and maintaining flexibility are fundamental treatments. Physiotherapy can help improve function, reduce pain, and slow progression of the condition.
Weight Management - Losing weight if overweight significantly reduces stress on knee joints and can improve symptoms considerably.
Pain Relief Medicines - Over-the-counter pain relievers like paracetamol and anti-inflammatory medicines (NSAIDs such as ibuprofen) can help manage pain and reduce inflammation. These should be used as part of a broader treatment plan.
Activity Modification - Adjusting activities to reduce impact on the knee, using walking aids if needed, and pacing activities can help manage symptoms.
Steroid Injections - Steroid injections are used when pain significantly limits function or prevents participation in physiotherapy and exercise programmes.
Other Injection Therapies - Hyaluronic acid injections (viscosupplementation) and platelet-rich plasma (PRP) are other options that may be considered, though evidence for their effectiveness varies. We do not presently offer these injections as we are unsure of effectiveness for knees.
Surgery - Joint replacement surgery (total or partial knee replacement) may be considered for severe osteoarthritis when other treatments have not provided adequate relief and quality of life is significantly affected.
How Steroid Injections Can Help
A steroid, usually combined with a local anaesthetic, is injected directly into the knee joint. The clinician uses anatomical landmarks to ensure accurate placement of the needle. The are numerous ways of approaching a knee injection, but we at The Edinburgh Joint Injection Clinic typically use an approach from the inner part of the knee.
Steroids work by reducing inflammation in the joint. Many people experience pain relief that allows them to engage more fully in exercise and physiotherapy, which are crucial for long-term joint health.
Research on steroid injections for knee osteoarthritis shows they provide short-term benefit, but they do have limitations. Studies demonstrate pain relief is most pronounced in the first 2-4 weeks after injection, and benefits can wear off by 8 weeks. The evidence suggests improvement occurs in approximately 50% of patients, though individual responses vary considerably. We have seen patients respond at both ends of the spectrum.
Long-term safety studies have shown that repeat injections every 3 months for up to 2 years appear safe without accelerating joint damage. Some recent research has raised some concerns about potential cartilage loss with repeated injections, though the clinical significance remains debated. For some patients who are too frail to consider definitive surgery, repeated injections can have a key role.
In short, steroid injections can provide meaningful short-term pain relief for many people with knee osteoarthritis, particularly those with inflammatory flares or effusions (fluid in the joint). However, they are not a cure, and should be part of a comprehensive treatment plan including physiotherapy, weight management, and other interventions.
What to Expect After a Steroid Injection
After an injection into the knee:
You may experience relief within a few days to a week
Maximum benefit typically occurs within 2-4 weeks
Relief usually lasts up to 8 weeks on average, though some get longer relief, particularly if the treatment is combined with physiotherapy
Exercise and activity modification remain important during and after the injection period
Summary
Knee osteoarthritis causes pain, stiffness, and reduced function due to cartilage breakdown in the joint.
Exercise, physiotherapy, and weight management are the cornerstones of long-term treatment.
Steroid injections can provide short-term pain relief for approximately 40-50% of patients, typically lasting 2-8 weeks.
Injections are most effective when used alongside exercise and other treatments, not as standalone therapy.
Response to injections varies considerably between individuals, and they work best when there is an inflammatory component to the pain.
If you are struggling with symptoms of knee osteoarthritis, you can contact us to discuss your needs, or book in directly for a consultation.
References
Jüni P, Hari R, Rutjes AW, Fischer R, Silletta MG, Reichenbach S, da Costa BR. Intra-articular corticosteroid for knee osteoarthritis. Cochrane Database of Systematic Reviews. 2015;Issue 10:CD005328.
Arroll B, Goodyear-Smith F. Corticosteroid injections for osteoarthritis of the knee: meta-analysis. BMJ. 2004;328(7444):869.
Raynauld JP, Buckland-Wright C, Ward R, et al. Safety and efficacy of long-term intraarticular steroid injections in osteoarthritis of the knee: a randomized, double-blind, placebo-controlled trial. Arthritis & Rheumatism. 2003;48(2):370-377.
Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care & Research. 2020;72(2):149-162.
McAlindon TE, LaValley MP, Harvey WF, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: a randomized clinical trial. JAMA. 2017;317(19):1967-1975.
This information is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your health provider with any questions you may have regarding a medical condition.
Privacy and GDPR Policy | Terms and Conditions for Website Use & Cookies
Dr. Peter Weil, MBChB, BSc, MRCGP (2007).
Registered with the Information Commissioners Office - ZB780390